Article Text

Abstract
Objectives Coal miners suffer increased mortality from non-malignant respiratory diseases (NMRD), including pneumoconioses and chronic obstructive pulmonary disease, compared with the US population. We characterised mortality trends from NMRD, lung cancer and ischaemic heart disease (IHD) using data from the Federal Black Lung Program, National Coal Workers’ Health Surveillance Program and the National Death Index.
Methods We compared mortality ORs (MORs) for NMRD, lung cancer and IHD in former US coal miners to US white males. MORs were computed for the study period 1979–2017 by birth cohort (<1920, 1920–1929, 1930–1939, ≥1940), with a subanalysis restricted to Central Appalachia.
Results The study population totalled 235 550 deceased miners, aged >45 years. Odds of death from NMRD and lung cancer across all miner birth cohorts averaged twice those of US males. In Central Appalachia, MORs significantly increased across birth cohorts. There was an eightfold increase in odds of death from NMRD among miners born after 1940 (MORBC≥1940 8.25; 95% CI 7.67 to 8.87). Miners with progressive massive fibrosis (PMF) were younger at death than those without PMF (74 vs 78 years; p<0.0001). We observed a pattern of reduced MORs from IHD in coal miners compared with national and regional counterparts.
Conclusion US coal miners have excess mortality from NMRD and lung cancer compared with total US and Appalachian populations. Mortality is highest in the most recent birth cohorts, perhaps reflecting increased rates of severe pneumoconiosis.
- Mortality
- Occupational Health
- Coal Mining
- Lung Diseases, Interstitial
Data availability statement
All data used in this study are owned and maintained by the US National Institute for Occupational Safety and Health and is not publicly available at this time.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Coal miners suffer excess morbidity and mortality from non-malignant respiratory diseases including pneumoconiosis and chronic obstructive pulmonary disease (COPD). Previous studies of mortality from ischaemic heart disease and lung cancer are inconsistent and have not examined historical trends.
WHAT THIS STUDY ADDS
We found that coal miners suffer from significantly increased odds of death from pneumoconiosis, obstructive lung disease and lung cancer compared with their counterparts in the US population. This higher mortality has also worsened over time and is especially severe in the Central Appalachian region of the USA. These findings are based on data from 235 550 deceased miners, the largest study of its kind to date.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Recent scientific and media attention has been focused on rising rates of pneumoconiosis, which is only the tip of the iceberg of diseases caused by coal mine dust. This study highlights the large burden of mortality due to COPD in coal miners, which may be caused by their occupational exposure. The increasing odds of death from these diseases in the most recent birth cohorts underscores the importance of controlling workplace exposures.
Introduction
Coal mine dust lung diseases (CMDLD) including coal workers’ pneumoconiosis (CWP), chronic obstructive pulmonary disease (COPD) and lung function impairment confer significantly increased risk for morbidity and mortality in affected workers.1–5 Earlier reports based on death certificates coded for pneumoconiosis showed that deaths from this disease in the USA decreased from 1968 to 2006, and cited more stringent dust regulations and declining coal mine employment (CME) as major reasons for this trend.6 7 Follow-up of one of these studies found that years of potential life lost per decedent had increased between 1999 and 2016, suggesting increased disease severity in recent decades.8 These studies were not based exclusively on populations of coal miners and did not address other non-malignant respiratory diseases (NMRD) such as COPD. Recent increases in CWP prevalence and its most severe form, progressive massive fibrosis (PMF),9–11 mainly within the Central Appalachian states of Kentucky, Virginia and West Virginia, may have led to reversal in this mortality trend.
Risk of death from malignant neoplasm has consistently been shown to be lower among cohorts of coal miners compared with the general population, but evidence for risk of death from lung cancer specifically is inconsistent.12 Despite occupational exposure to known carcinogens such as diesel exhaust particulates, radon and crystalline silica, early reports found no evidence of increased lung cancer mortality among US coal miners.1 5 These studies may have been confounded by differences in geologic features between mines, in coal mine dust constituents, in mining methods and dust controls used, and in individual mining job duties and tasks. These studies also have relatively small sample sizes of lung cancer cases or short periods of longitudinal follow-up. Two extended follow-up examinations of US and British cohorts of coal miners demonstrated elevated lung cancer risk associated with increased occupational exposure to silica dust.2 3
Cardiovascular disease mortality risk among coal miners is also an area of growing interest. An early study of heart disease mortality among 3726 US Appalachian coal miners found a significant reduction in risk of death from ischaemic heart disease (IHD) compared with the Appalachian population as a whole, though currently smoking miners had an increased risk of IHD mortality.13 Lower IHD mortality has been reported in Japanese and British coal mining cohorts, attributed to the healthy worker effect.3 4 Risk of death from IHD was not consistent over four time periods examined in Dutch coal miners, with initial increases in risk of IHD mortality tapering off after the latest follow-up period.14 In contrast, Landen et al reported significantly increased risk from IHD with increasing cumulative respirable coal mine dust exposure among a US miners, after controlling for age, smoking and body mass index.15
In the USA, the two largest sources of health data on coal miners are the Coal Workers’ Health Surveillance Program (CWHSP) administered by the National Institute for Occupational Safety and Health (NIOSH) and the Federal Black Lung Program (FBLP) administered by the Department of Labor (DOL), both established in 1969. The CWHSP primarily screens active miners for radiographic disease and lung function impairment, with the goal of secondary prevention of CMDLD.16 The FBLP provides compensation and medical coverage to coal miners who are totally disabled by CMDLD.17 These data were recently linked18 and show promise for tracking health trends and disease risks in US coal miners during and after their CME.
The current study aims to characterise causes of death among US coal miners who have participated in either programme and to examine mortality trends by age and birth cohort, with particular focus on mortality from NMRD, lung cancer and IHD. The large population of miners in this study allows examination of mortality trends in Central Appalachia, which has experienced the largest increase in CWP and PMF prevalence in recent decades. Better understanding of disease trends in this high-risk worker population will help inform targeted exposure prevention and early disease detection strategies.
Methods
Data sources
We obtained vital status and cause of death data from Social Security Administration and National Death Index (NDI) sources on US coal miners who participated in either the CWHSP or the FBLP. A Memorandum of Understanding was established between DOL and NIOSH for access to FBLP claims made in 1 January 1970–31 December 2017. CWHSP participants from 1970 to 2017 were included to maximise the number of records we could link to the FBLP data.
We requested mortality data on all deceased miners from either programme from the NDI who were known to be deceased using Social Security Administration vital status queries performed by either the DOL or NIOSH on their respective populations. Additional records of CWHSP miners were submitted with unknown vital status. We submitted names, dates of birth (DOB), Social Security numbers (SSN), and, where available, sex and race to the NDI.
Mortality data from the general US population from 1979 to 2017 was obtained from the National Vital Statistics System (NVSS) through publicly available and special request data files. Special request data files were necessary to obtain state of death which was unavailable in NVSS data since 2004.19 Relevant to our study, NVSS data included underlying cause of death, age at death, year of birth and state of death. Cause of death was coded using the International Classification of Diseases (ICD)-9 for years 1979 to 1998, and ICD-10 for years 1999–2017.
National Death Index
The NDI employs a probabilistic linkage procedure to identify death records that are potential matches to submitted data. We included all NDI records that were exact matches of first and last names, SSN and DOB to a death certificate file in their database. We also included records requiring one of the following: an exact nine-digit SSN match; an eight-digit SSN match and an exact DOB match or a seven-digit SSN match and an exact DOB match.20
The NDI provides underlying and contributing causes of death for matched records. In addition to the underlying cause of death, a maximum of 20 additional conditions that contributed to the death (contributing causes) were provided by the NDI.
Selected causes of death
We examined selected underlying and contributing causes of death including NMRD, lung cancer and IHD. We examined subcategories of NMRD including pneumoconioses and chronic lower respiratory disease (CLRD). NMRD was identified using ICD-9 codes 460–519 and ICD-10 codes J00–J99. We identified pneumoconioses other than asbestosis, which includes CWP, silicosis and pneumoconiosis resulting from exposure to inorganic dusts, using ICD-9 codes 500, 502, 503, 505 and ICD-10 codes J60–J62, J64. CLRD, including COPD, chronic bronchitis, emphysema and asthma, was identified using ICD-9 codes 490–494 and 496; and ICD-10 codes J40–J47. We defined lung cancer as ICD-9 code 162 and ICD-10 code C34. We identified IHD, including acute myocardial infarction and chronic IHD, using ICD-9 codes 410–414 and ICD-10 codes I20–I25.
Statistical analysis
We characterised proportional mortality from selected underlying causes of death, employing χ2 tests and logistic regression to test for significant trends across birth cohort and age group. Causes of death examined were NMRD, pneumoconioses excluding asbestosis, CLRD, lung cancer and IHD. We also examined differences in mortality trends between those with and without a determination of PMF from the FBLP adjudication process. This determination process has been described previously,21 and reflects the DOL’s determination of whether the miner has PMF based on medical evidence submitted with their claim.
We computed mortality ORs (MORs) to compare mortality from all NMRD, pneumoconioses, CLRD, all malignant neoplasms, lung cancers and IHD among former US coal miners and the US white male population.21 MORs represent the ratio of odds of death from a specific cause in the study population to odds of death from that specific cause in a comparison population.22 23 MORs were computed for the entire study period of 1979–2017 by birth cohort (<1920, 1920–1929, 1930–1939 and ≥1940), as well as by age group within birth cohorts (<65 years, 65–74 years, and 75 years and older). We also calculated MORs for a subgroup of miners, restricting analysis to miners who last worked in a Central Appalachian state. All analyses were restricted to those aged 45 and older at the time of death.
Results
Study population
Of the 353 547 records submitted to the NDI, 239 361 (67.7%) were identified as having a match in the NDI database. Of the 114 186 miners without a match in the NDI, 72% (n=81 886, all from the CWHSP) were presumed to be still alive. Of the remaining 32 300 presumed deceased miners, 6.3% (n=2028) had obvious errors in their DOB, indicated by a miner’s age at death being younger than their age at the time of filing their FBLP claim. This suggests that 30 272 miners (8.6% of all miners submitted to the NDI) had errors in key matching variables submitted to the NDI, chiefly first and last names, SSNs and DOB. These miners were more likely to be from the earliest birth cohort (85.5% born before 1920), with unknown tenure (50.6%) and region of mining (53.7%).
Excluding those aged <45 years, a total of 235 550 US coal miners were included in the final dataset. Mean age at death was 76 years (SD 10.6 years). The majority of miners were born before 1929 (67.5%; table 1). Forty-three per cent worked their longest-held mining tenure in Central Appalachia (Kentucky 14.1%; Virginia 6.7%; West Virginia 22.3%). Certified years of CME were only available for a subset of miners who applied for benefits through the FBLP (n=1 36 679, 58%). Mean CME in this group was 19 years.
Descriptive characteristics of deceased miners, aged 45 and older at time of death (n=235 550), participating in the Coal Workers’ Health Surveillance Programme or applying for Federal Black Lung Programme benefits, 1970–2017, by PMF status.
The most common underlying causes of death in this population were IHD (25.0%), NMRD (20.4%), malignant neoplasms excluding lung cancer (12.6%) and lung cancer (9.7%) (table 1). Among those with NMRD as the underlying cause of death (n=47 932), the two most prevalent causes were COPD (n=20 185, 42.1%) and pneumoconiosis (n=17 207, 35.9%). Not surprisingly, CWP accounted for 86.2% of those with pneumoconiosis listed as the underlying cause of death. Unspecified pneumoconiosis comprised an additional 11.5% of these cases, and pneumoconiosis arising from exposure to silica dust was cited in only 2.5% of these cases.
There were 2829 miners who were determined to have PMF by the DOL adjudication process.24 Miners with PMF were significantly younger at the time of death than those without this determination (74 and 78 years, respectively; p<0.0001). A significantly higher proportion of PMF miners were born in the most recent birth cohorts (1930 and after; 32.6%) compared with non-PMF miners (14.1%; p<0.0001, table 1). Among miners with PMF, 56.1% worked in Central Appalachia and 28.6% worked in Pennsylvania. Of the remaining PMF cases, most arose in miners working primarily in Ohio (3.7%), Alabama (2.8%), Tennessee (1.9%) and Illinois (1.6%).
Pneumoconioses were listed as the underlying cause of death in 7.3% of the study population, and as a contributing cause of death in 18.9%. When examined by PMF determination status, pneumoconioses were indicated as the underlying cause of death in 19.3% of PMF miner deaths and only 7.2% of miners without a PMF determination. PMF miners were significantly more likely to have NMRD listed as the underlying cause or as a contributing cause of death than non-PMF miners. Only 37.5% of PMF miners had pneumoconiosis listed as a contributing cause of death on their death certificates.
Mortality ORs
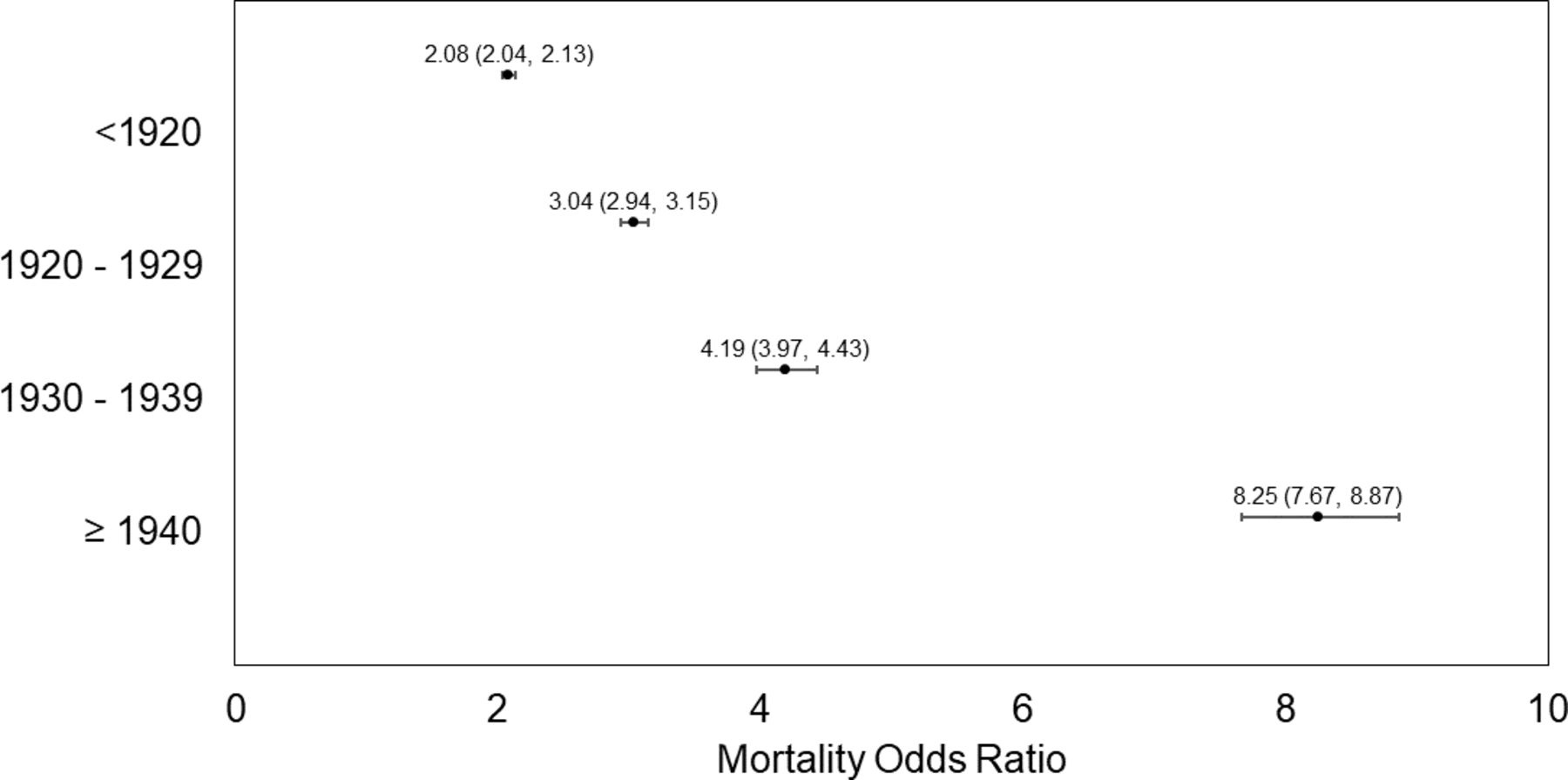
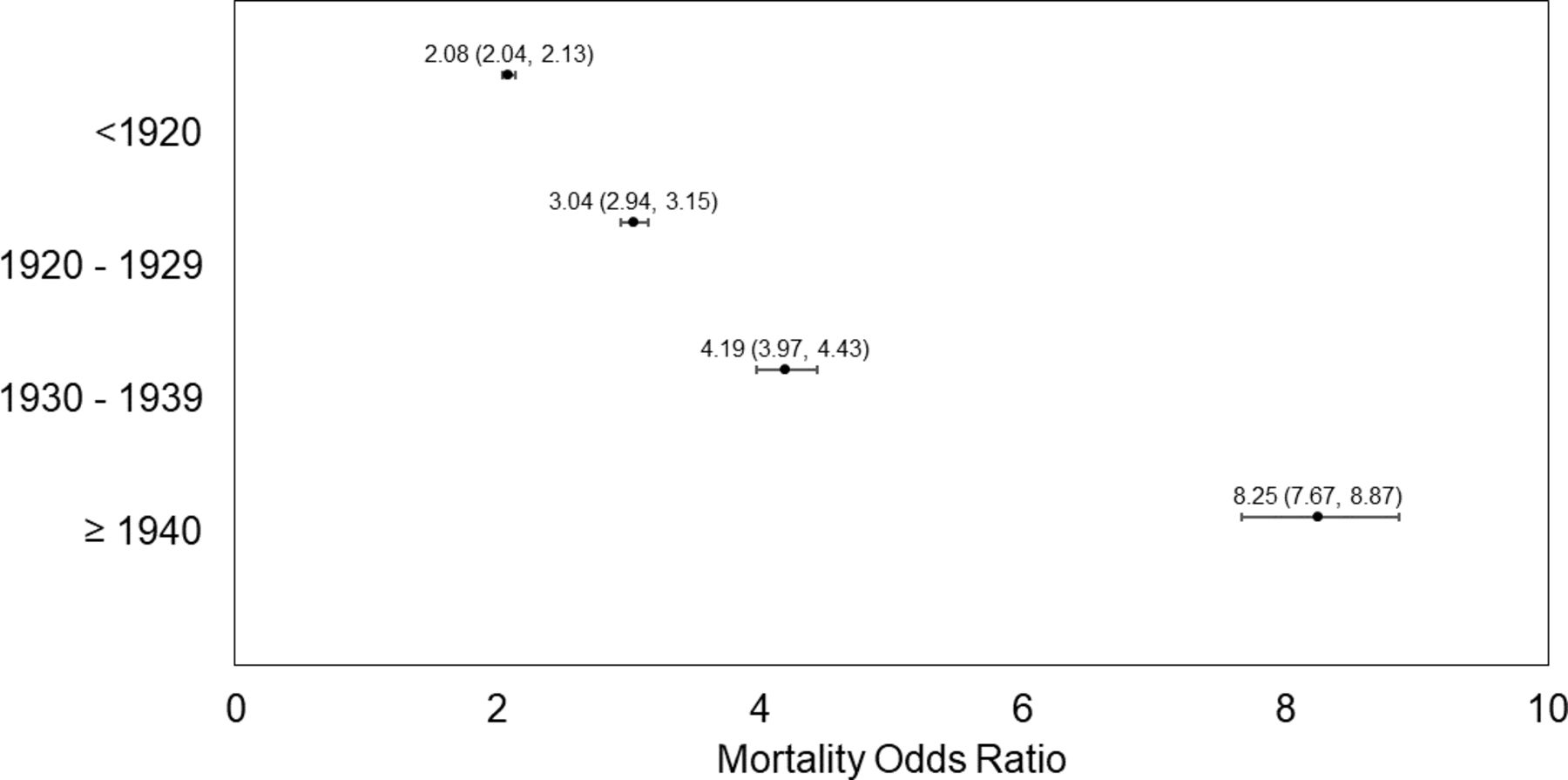
The odds of death from NMRD across all birth cohorts of coal miners in this population were, on average, twice as high as those of the US population of white males aged 45 years and older (table 2). In Central Appalachia, MORs for NMRD significantly increased across successive birth cohorts. There was an eightfold increase in odds of death from NMRD among miners born after 1940 (MORBC≥1940 8.25; 95% CI 7.67 to 8.87), compared with the general Central Appalachian population (figure 1).
{kind=link}
Mortality ORs (MORs) from non-malignant respiratory disease among coal miners compared with non-coal miners in central Appalachia by birth cohort. Population restricted to those aged 45 and older at time of death. MOR point estimates and their 95% CIs are included.
Mortality ORs and 95% CI, by birth cohort, for selected underlying causes of death among a population of deceased US coal miners (n=235 550) and the general US population of white males, for deaths occurring among persons 45 years and older who died 1979–2017.
In contrast, MORs for NMRD were lower for the cohort of miners born after 1940, but remained significantly elevated. Odds of death from NMRD were highest in the youngest age group (<65 years) in all birth cohorts except those born between 1930 and 1939 (table 3).
Mortality ORs from selected causes of death by age group and birth cohort among 235 550 deceased US coal miners participating in the federal Coal Workers' Health Surveillance Programme or applying for Federal Black Lung Programme benefits, 1970–2017
Odds of death from pneumoconioses were between 149 and 658 times that of the US population, depending on age group and birth cohort. Pneumoconiosis MORs were unstable in Central Appalachia due to small numbers in the US population (data not shown).
All birth cohorts of miners had significantly elevated odds of death from lung cancer compared with the non-mining US population of non-Hispanic white men (table 2). In Central Appalachia, the likelihood of lung cancer mortality was significantly elevated among the earliest and latest birth cohorts (MORBC<1920 1.31; 95% CI 1.27 to 1.35; MORBC≥1940 1.14; 95% CI 1.07 to 1.21; table 2). All age groups of miners had significantly elevated odds of death from lung cancer except the oldest miners in the most recent birth cohort, likely a reflection of the small sample size (table 3). We found no evidence of increased odds of mortality from all malignant neoplasms in either the national or Central Appalachian analyses. Nationally, most birth cohorts showed significantly reduced odds of death from malignant neoplasms in coal miners compared with the non-mining US population (table 2).
Central Appalachian miners had significantly lower odds of death from IHD compared with their non-mining counterparts, with each successive birth cohort experiencing lower odds of death from this cause (MOR range 0.72–0.93; table 2). Nationally, there were significant reductions in odds of IHD mortality in most strata of age and birth cohort (table 3).
Discussion
This study characterises the changing burden of mortality from NMRD, IHD and lung cancer across birth cohorts in the largest mortality study of US coal miners to date. To place the scale of this study of 235 550 miners in context, previous mortality studies of coal miners examined cohorts of 3729–18 666 miners.1–3 13 15 Nationally, we found increased odds of mortality from NMRD, including from pneumoconioses and chronic lower respiratory diseases such as COPD, across all birth cohorts examined. Within Central Appalachia, the odds of death from NMRD increased significantly across birth cohorts, with the highest odds seen in the most recent birth cohort of miners. This may reflect increased mortality from PMF, which is occurring more frequently and in younger Central Appalachian coal miners.10 11 This hypothesis is further supported by our findings that a significantly higher proportion of miners with PMF were born in the most recent birth cohorts (1930 and after; 32.6%) compared with non-PMF miners (14.1%) and that the majority of PMF miners in our study worked in Central Appalachia. Miners with PMF were significantly younger at the time of death than those without this determination.
To our surprise, we discovered that, of miners with PMF, only 37.5% had pneumoconiosis listed as a contributing cause of death on their death certificates despite all of these miners undergoing standardised pulmonary assessments by certified physicians. These findings suggest that the designation of ‘pneumoconiosis’ as a cause of death likely does not reflect the true burden of dust-related lung disease mortality in this population, and that other ICD terms (eg, NMRD) may subsume a substantial number of deaths from occupational pneumoconiosis.
NMRD includes pneumoconioses (CWP and silicosis) as well as other chronic lower respiratory diseases. We found consistently and significantly elevated odds of death from chronic lower respiratory diseases, the majority from COPD, among coal miners compared with their US counterparts across every birth cohort and in nearly every age group nationally and within Central Appalachia. These findings are consistent with previous mortality studies of US coal miners and underscore the importance of coal mine dust as a cause of occupational COPD.1 2 The increased odds of death from pneumoconiosis among our cohort of miners compared with the US population were orders of magnitude higher than most other associations we observed. Each of the 17 207 deaths in which pneumoconiosis was the underlying cause of death was entirely preventable, caused by overexposure to coal mine dust. Our findings support the well-established link between coal mining and risk of death from pneumoconiosis.1–5 14
Coal miners face potential exposure to known carcinogens in their work environment including diesel exhaust, silica, asbestos and radon. Nationally, we found across all four birth cohorts that coal miners had significantly increased odds of death from lung cancer compared with the general US population. In Central Appalachia, this association was significantly elevated in the earliest and most recent birth cohorts. Our findings support the growing literature that coal miners are at risk of increased mortality from lung cancer, particularly among those with increased exposure to silica dust.2–4 A recent study of regulatory dust monitoring data from 1980 to 2017 revealed that the percentage of silica-containing respirable dust was significantly higher in Central Appalachian underground mines compared with those in the rest of the USA.25 This time frame encompasses much of the working careers of miners in the most recent birth cohort in our study.
The USA has experienced a decrease in IHD mortality since its peak in 1968.26 27 This has been attributed to reductions in cigarette consumption, treatment of hypertension and increased use of medications for primary prevention of acute cardiovascular events. This national trend was accentuated in our study population through the significant reduction in proportional mortality from IHD across time. We observed significantly lower odds of mortality from IHD among Central Appalachian coal miners compared with their white male counterparts in the general population, consistent with other studies that found significantly reduced mortality from IHD among coal miners attributable to the healthy worker effect.1 3 4
One strength of this study was examining selected mortality outcomes within Central Appalachian states that comprised 43% of our study population and have distinct exposures and socioeconomic challenges. Previous literature demonstrates increased incidence of and mortality from heart disease28 and malignant neoplasms including lung cancer29 30 in Appalachia compared with the rest of the USA. Cardiopulmonary disease risk factors such as obesity and cigarette smoking are also found at elevated rates in Central Appalachia.31 32 The Central Appalachian subanalyses have greater potential to control for confounding risk factors in the general population.
A major study limitation was lack of data on smoking habits. Smoking data are not systematically collected or reported by either the CWHSP or FBLP. Consequently, we were unable to assess the role of smoking rates on changes in mortality. Current cigarette smoking rates declined dramatically between 1965 and 2017 in the USA, from 52.0% to 15.8% among men and from 34.1% to 12.2% among women.33 National data obscures state differences, notably in Central Appalachia where smoking rates remain high. Based on 2014–2015 data from the US Current Population Survey, the prevalence of current cigarette use is 21.1% in Kentucky, 13.2% in Virginia and 21.7% in West Virginia.34 Even state-wide estimates may mask within-state regional differences, with one study reporting current cigarette use in 2010 in the Appalachian counties of Kentucky as 30.9% compared with 24.3% in non-Appalachian counties.31
While smoking rates have declined among the general US population, tobacco use among miners remains high. The prevalence of current cigarette use in the US mining industry is 25.2%, and these workers have nearly twice the odds of using tobacco products compared with other workers.35 Consistent with state and regional estimates, we assumed that cigarette smoking rates among coal miners in this study are likely high but comparable to their regional counterparts. Further, odds of death from IHD in miners were lower than their non-coal mining counterparts, suggesting that cigarette smoking likely does not explain the observed increased odds of death from NMRD or lung cancer among the miners in this study. This is important since even modest smoking (one cigarette/day) increases heart disease risk by almost 50%, with 1 pack/day doubling the risk.36 If there was substantially greater tobacco smoking among miners than the general population, we should have observed elevated MORs for IHD.
An additional study limitation is the reliance on death certificate classifications of causes of death. As expected, miners with a determination of PMF by the FBLP were significantly more likely to have pneumoconiosis listed as cause of death, but only 29% of PMF-miners had CWP listed on their death certificate. Part of this discrepancy may be explained by limitations of the death certificate coding process. Death certificates include contributing cases of death rather than all conditions present at the time of death.37 It is possible that pneumoconiosis, while present in those with a determination of PMF, was not the cause of death for some individuals. Further, causes of death on death certificates reflect opinions of the medical certifiers and can vary based on that certifier’s training, experience and access to medical histories and autopsy or diagnostic test results. Correct identification and recording of pneumoconiosis as a cause of death may vary by region and familiarity of medical examiners with the disease and the decedent’s occupation, a phenomenon seen in other populations with occupational lung disease.37–39 Altogether, our findings suggest that the number and proportion of deaths in which pneumoconiosis was a contributing cause is under-reported in this study.
Finally, the datasets used in this study do not capture the full universe of US coal miners which may limit generalisability. However, the US Centers for Disease Control and Prevention publishes proportional mortality data for selected industries, and their data are consistent with ours in finding elevated mortality from pneumoconioses, COPD and lung cancer among white males in the coal industry.40
Conclusions
US coal miners experience excess mortality from respiratory diseases including pneumoconiosis, chronic lower respiratory diseases and lung cancer, compared with total US and Central Appalachian populations. Of great concern, these associations are highest in the most recent birth cohort, consistent with increasing rates of CMDLD and PMF. This study highlights the increased relative contribution of obstructive lung disease to CMDLD mortality and underscores the importance of coal mine dust exposure as an important cause of occupational obstructive lung disease.
Data availability statement
All data used in this study are owned and maintained by the US National Institute for Occupational Safety and Health and is not publicly available at this time.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the NIOSH institutional review board (IRB protocol ID: 16-RHD-05XP).
References
Footnotes
Contributors KSA contributed to the conceptual design, methods development, and data acquisition for this manuscript. She performed all data management, cleaning and analyses; as well as drafted and revised the manuscript. She is guarantor of this manuscript. CNH was instrumental in the project conceptualisation and data acquisition for this work. She also aided in manuscript revisions. LSF helped develop the analytic approach to these data and aided in manuscript preparation and revisions. CSR, NBH and LHTG contributed to data interpretation, manuscript preparation and revision. RAC contributed to all aspects of project conceptualisation, methods development, data acquisition, data interpretation, and manuscript preparation and revision.
Funding This research was supported in part by National Occupational Research Agenda intramural funding from the National Institute for Occupational Safety and Health and a grant from the Alpha Foundation for the Improvement of Mining Safety and Health (#AFCTG20-102).
Disclaimer The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention. The views, opinions and recommendations addressed here are solely those of the authors and do not imply any endorsement by the Alpha Foundation, its Directors and staff.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.